Testing if a patient can actively extend both knees and achieve at least a 3/5 grade knee extensor strength on Oxford scale is a basic way of assessing their capacity to attempt a sit to stand or gait.
The most obvious cause for an acute reduction in haemoglobin is haemorrhage! i.e. bleeding
(I'm writing this because I was asked today and stupidly searched for some kind of complex cause and in doing so failed to come up with the most likely cause!)
This could be internal bleeding e.g. peptic ulcer or inflammatory bowel disease as well as external bleeding from a haemorrhage
Hemolysis
Kidney disease
One of the functions of the kidney is to produce a hormone called erythropoeitin which signals the bone marrow to produce red blood cells. Kidney disease can result in reduced levels of this hormone causing chronic anemia (according to livestrong)
If a patient has thrombocytopenia AKA low platelet count then medicines such as: ibuprofen and aspirin should be ceased as these have the potential to cause GI bleeds.
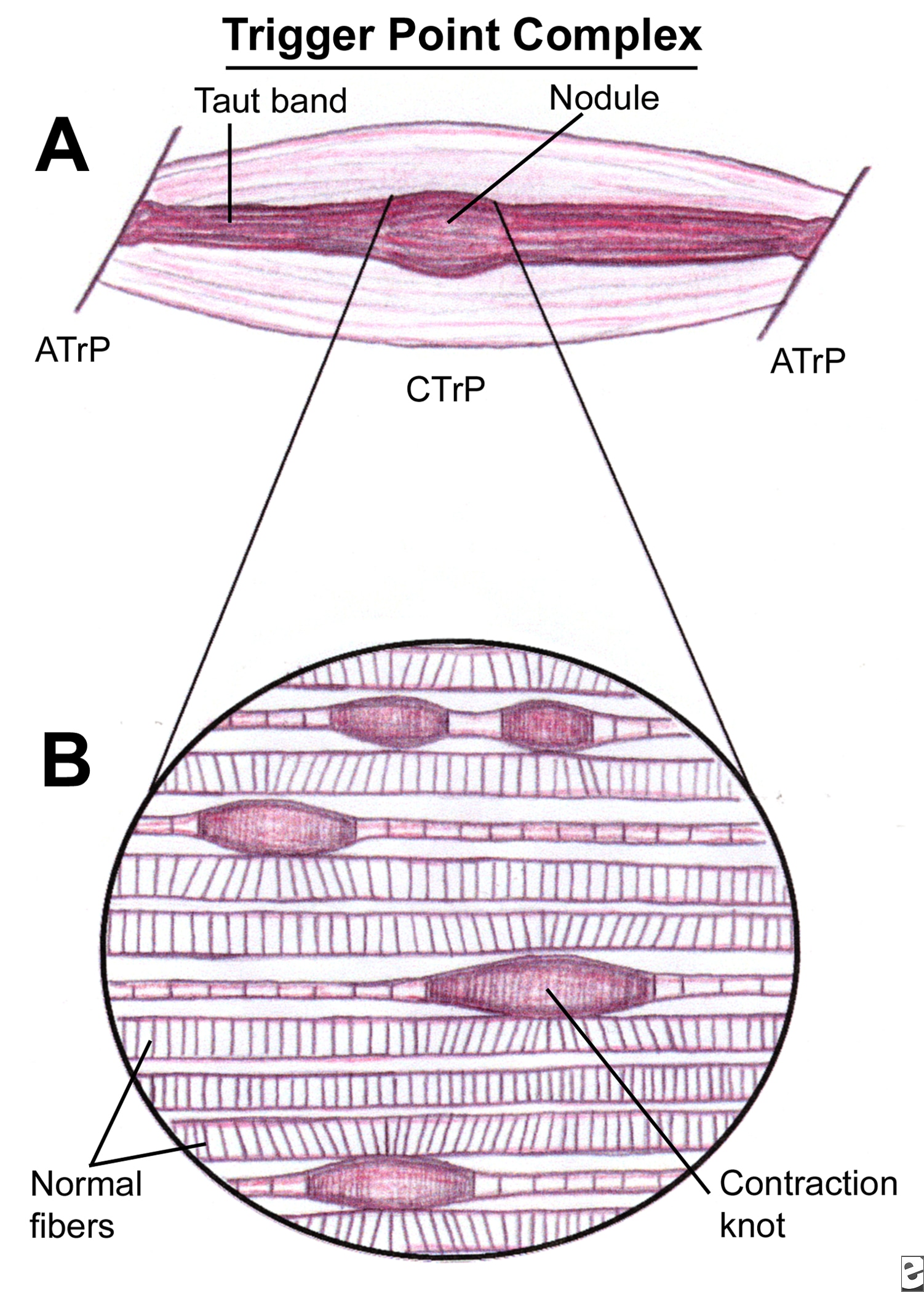
A focal hyperirritable spot in skeletal muscle associated with a palpable nodule in a taut band: painful on compression and can give rise to characteristic referred pain; tenderness; motor dysfunction and autonomic phenomena (Simons et al., 1999).
Definition 2.
"A trigger point is an area of the soft tissue which, after chronic contraction and reduced blood flow, becomes an area of high neurological activity. For example, fibers in an ischemic muscle (a muscle with low blood) can become an active trigger point in response to biochemical changes in the tissue. Active trigger points cause referred sensation to other parts of the body." www.painreliefvermont.com
Phases of Trigger Points (American Academy of Manual Medicine)
1. Active Trigger Point - Palpable nodular mass within muscles, fascia, scar tissue, ligaments, and periosteum. Produces a subjective referred pain complaint or autonomic phenomena, which is present constantly regardless of activity or rest.
2. (Same as above) produces a subjective referred pain or autonomic phenomena during activity but reduced or eliminated through rest.
3. Latent Trigger Point - (Same as above) but when snapped transversely it may replicate a referral pattern as if it were active. Without direct pressure, it does not produce a subjective referred pain or autonomic phenomena during either activity or rest.
4. Muscle tissue that does not exhibit a palpable ropy or button like nodular mass (characteristic of a TrP). However, the tissue may be hypertonic effecting ROM, structural deviation, and hypersensitive to tactile pressure.
Aetiological factors (what can cause them?) Travell and Simons (1999)
Direct stimuli = Maggie Simpson Resists Talking
Mechanical overload
Sudden cooling of fatigued muscles
Repetitive usage resulting in fatigue
Trauma
Indirect stimuli = My Other VAN MET IN EGYPT
Myopathy
Other TrPs which activate secondary triggers
Visceral Disease
Arthropathy
Neuropathy
Metabolic dysfunction
Endocrine dysfunction
Toxicity
Infection
Emotional Distress
How can I treat them?
Good thing about trigger points is that they're predominantly self-treatable and also treatable with massage.
Lacrosse ball! (Check out this clip with Kelly Starrett going through some lower limb demonstrations of how to use the lacrosse ball for self-myofascial release)
Ischaemic compression (While the thumbnail of this vid looks dodgey as hell the explanation of this technique is useful in getting a better idea of how it fits in with what's going on at tissue level. There is no explanation about why he has his shirt off as well?!)
To make up for that last video, here's a chiropractor talking about locating pec minor/major trigger points.
These are just a couple of techniques that can be used. Pettrisage, deep stroking, vibrations are other ways of resolving trigger points but essentially the desired effect is the same, regardless of what technique you use: facilitate localised lymphatic drainage and enhance the flow of oxygenated blood (and therefore nutrients) to the ischaemic area of tissue. Also, as Kstar mentions the video above, we want to improve the ability of the muscle, fascia, nerves etc to slide along the mechanical interfaces of each other to allow for smooth full ROM at each joint.
To finish, Claire Davies uses an analogy that I really find helpful comparing trigger point release to wringing out a wet cloth. A repetetive 'milking' action to rinse out the dirt until fresh water can run through clear (Davies, 2002).
Davies, C (2002) Massage & Bodywork Magazine, Associate Bodywork and Massage Professionals.
Simons, D., Travell, J., Simons, L (1999) Myofascial Pain and Dysfunction: Upper half of body, Lippincott Williams & Wilkins.
This is when the muscle contracts at a constant speed and max effort through the full ROM. This can be achieved by a therapist when either assessing or treating by applying an active resistance to the patient/client but allowing them to overcome this at a certain speed through the entire range. A KIN-COM machine achieves the same effect, permitting the muscle to contract whilst keeping the same max force/rate movement through range (therefore building strength through range).
ISOTONIC
The force/tone remains constant BUT speed can vary. This speed can vary based on lever length.
Disadvantage is isotonic training is that because there's that potential for variability muscles can develop predominantly in only the area where the most force is applied.

 A focal hyperirritable spot in skeletal muscle associated with a palpable nodule in a taut band: painful on compression and can give rise to characteristic referred pain; tenderness; motor dysfunction and autonomic phenomena (Simons et al., 1999).
A focal hyperirritable spot in skeletal muscle associated with a palpable nodule in a taut band: painful on compression and can give rise to characteristic referred pain; tenderness; motor dysfunction and autonomic phenomena (Simons et al., 1999). 
 The force/tone remains constant BUT speed can vary. This speed can vary based on lever length.
The force/tone remains constant BUT speed can vary. This speed can vary based on lever length. 